What are varicose veins?
What are varicose veins?
Varicose veins are thick and lumpy superficial veins of the lower limbs. Venous valves in the veins prevent blood backflow (falling due to gravity). In varicose veins, these valves are destroyed. Repeated to-and-fro blood flow in the veins causes symptoms such as swelling of the legs, pain, pigmentation, and skin ulcers (Fig. 1). Leg cramps are one of the most painful symptoms. The edematous lower leg due to the blood stasis is like a mud flood, where muscles lack oxygen and can cause cramps.

Concept of treatment
Superficial veins (great saphenous vein: inside the thigh, small saphenous vein: lower leg and back of the knee) with collapsed valves cannot return blood to the heart and cause the above symptoms. Surgeries include “stripping” (cutting and pulling them out) and “laser ablation” (burning them from the inside with a laser). “Deep” veins function fully for blood circulation in the lower limbs even if there are no superficial veins. During these surgeries, compression therapy is the basic therapy. Compression from the outside crushes the superficial veins and only the “deep” veins function; thereafter, most of the symptoms disappear. Elastic stockings have the disadvantage of being hard and difficult to wear, but they have been improved steadily recently (Fig. 2).

Laser / radio high-frequency ablation and stripping surgery
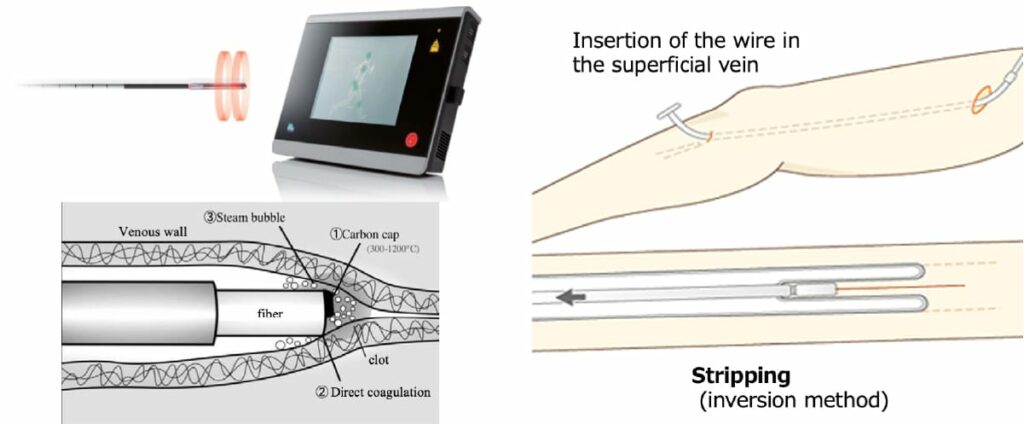
The conventional stripping technique (inserting a wire into the saphenous vein and pulling it out) and laser or radio high-frequency ablation (cauterizing the inside of the vessel) are currently performed (Fig. 3). Varicose vein surgery is minimally invasive and requires at most 2 or 3 days of hospital stay. Since the ablation was approved by health insurance institutions, it has been performed at many facilities. One-day surgery at the clinic can now be done “easily.” However, is it really “easy?” Is it safe?
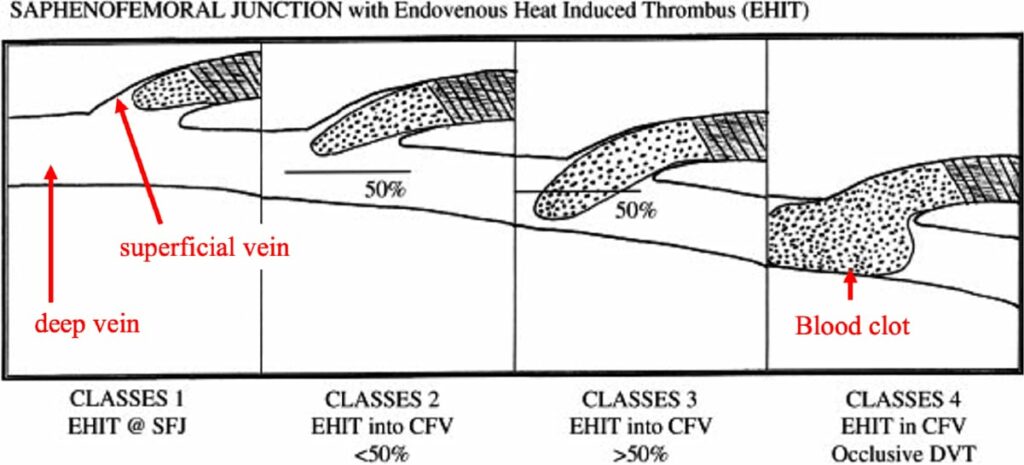
There is a complication called endovenous heat-induced thrombosis (EHIT). The ablation results in a blood clot in the vein as a result of cauterization. Usually, the proximal tip of the clot should be placed 1–2 cm below the safeno-femoral junction after the procedure. When the tip protrudes into the deep vein, it might cause deep vein thrombosis and/or pulmonary embolism (Fig.4). Considering the risk of EHIT, we perform ultrasonography on the same day, after surgery. In addition, we check the spread of the hematoma and the state of leg inflammation. Therefore, we ask patients to stay in the hospital for one or two nights as we believe that safety is more important than convenience.
Types of varicose veins of the lower leg
Besides the above-mentioned so-called varicose veins (primary varicose veins), varicose veins include congenital ones (i.e., Klippel-Trenaunay syndrome), and various secondary varicose veins (dilatation/various changes of superficial veins via increased blood flow due to deep vein thrombosis or arteriovenous fistula [AVF]). If it is primary, there is no problem with the above surgeries; however, if it is secondary, the surgeries are contraindicated because the superficial (varicose) veins are indispensable routes of venous return. Before surgery, it is necessary to carefully check the deep vein besides the target superficial veins using ultrasonography.